02 – HSD vs AltitudexTime
Two sessions at the same
altitude can produce
radically different dose.
Across the 18-session block, HSD and the conventional km·hrs metric diverge sharply. Sessions with identical altitudextime exposure produce up to 3x differences in HSD – driven by individual desaturation depth that altitude alone cannot see.
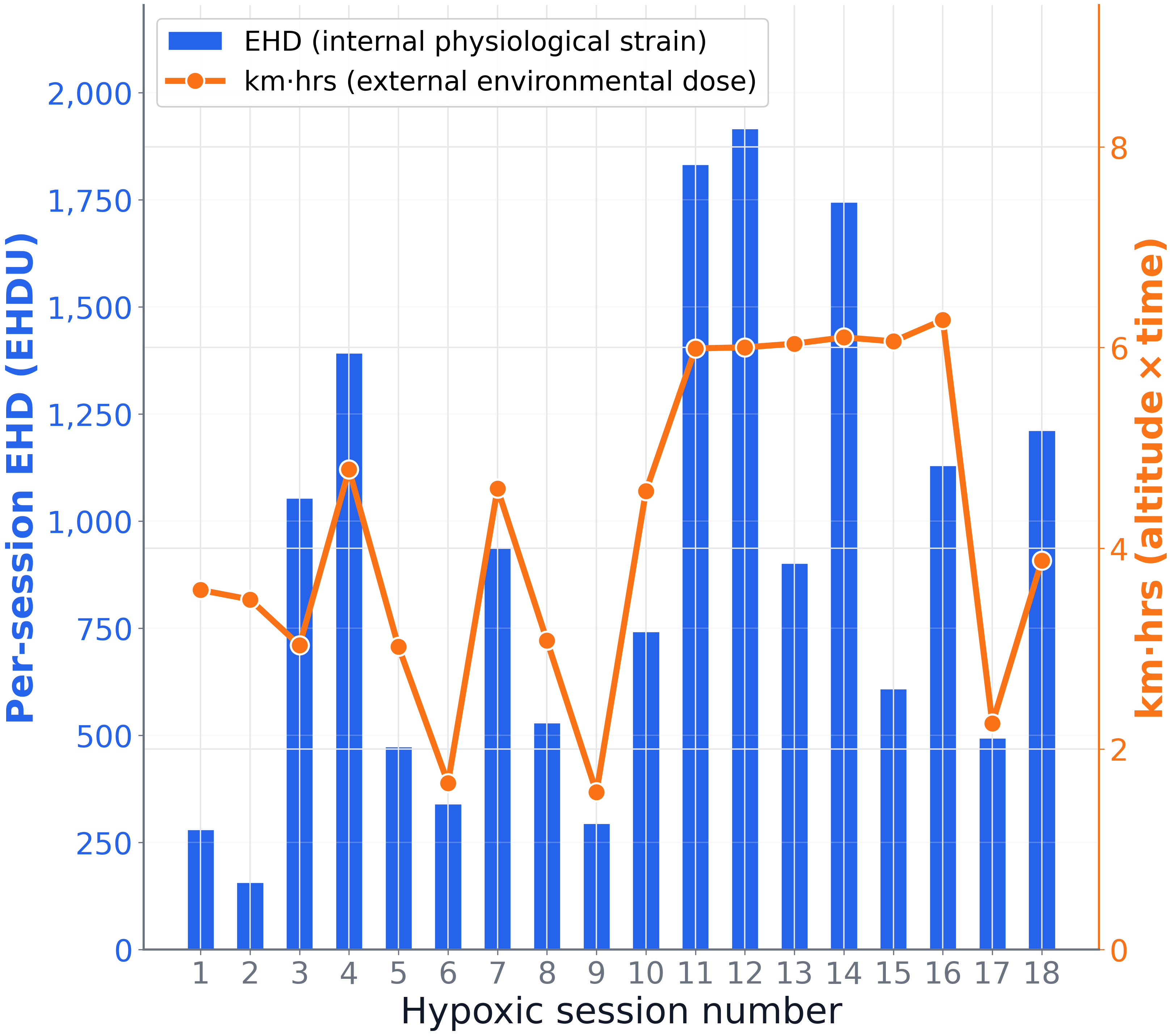
Per-session HSD (blue, internal hypoxic stimulus) vs km·hrs (orange, external environmental dose) across 18 IHT sessions. Where the two diverge, an altitudextime measure misses the physiological reality.